hypertrophic cardiomyopathy
Echocardiography Textbook
Hypertrophic cardiomyopathy is diagnosed when there is unexplained hypertrophy of the myocardium. The disease is most often caused by genetic changes in sarcomeres. More than 50% of cases are autosomal-dominant.
Echocardiography is one of the most important methods for diagnosing hypertrophic cardiomyopathy. It detects the corresponding changes in the myocardium and excludes other possible causes of hypertrophy.
According to the nature of hypertrophy, hypertrophic cardiomyopathy can be of the following types:
- Asymmetric hypertrophy of the interventricular septum (the most frequent variant) is usually predominantly hypertrophied in its basal part.
- Symmetrical - symmetric hypertrophy of the entire left ventricle (concentric).
- Hypertrophy of the basal part of the interventricular septum (sigmoid septum).
- Hypertrophy of the apical part of the interventricular septum.
- Hypertrophy of the middle part of the ventricular cavity or papillary muscles (very rare, usually accompanied by intraventricular obstruction).
Hypertrophic cardiomyopathy can be:
- Obstructive: systole with obstruction of the outflow tract of the left ventricle.
- Non-obstructive: without obstruction.
Hypertrophic cardiomyopathy is characterized by a decrease in the volume of the left ventricle and dilatation of the left atrium.
Systolic function is either normal or increased. Often, the ratio of the thickness of the interventricular septum to the thickness of the posterior wall is greater than 1,3.
Diastolic dysfunction is noted in approximately 80% of patients.
In about a quarter of patients, there is a narrowing of the left ventricular outflow tract. The result is its dynamic obstruction. Pre-systolic movement of the mitral valve leaflets (especially the anterior leaflet), prolongation of the leaflets, and changes in the subvalvular apparatus - contribute to the obstruction of the outflow tract. The contact point of the mitral valve cusps is located in the middle of their body, not at the ends.
A midsystolic change in flow velocity through the aortic valve causes vibration of its leaflets, which can also be detected on a one-dimensional echocardiogram.
Spectral continuous wave Doppler is the best method for investigating dynamic obstruction. Flow velocity in the LV outflow tract is increased and is characterized by a late peak (maximum velocity is reached at the end of systole) with a sharp end and asymmetric character.
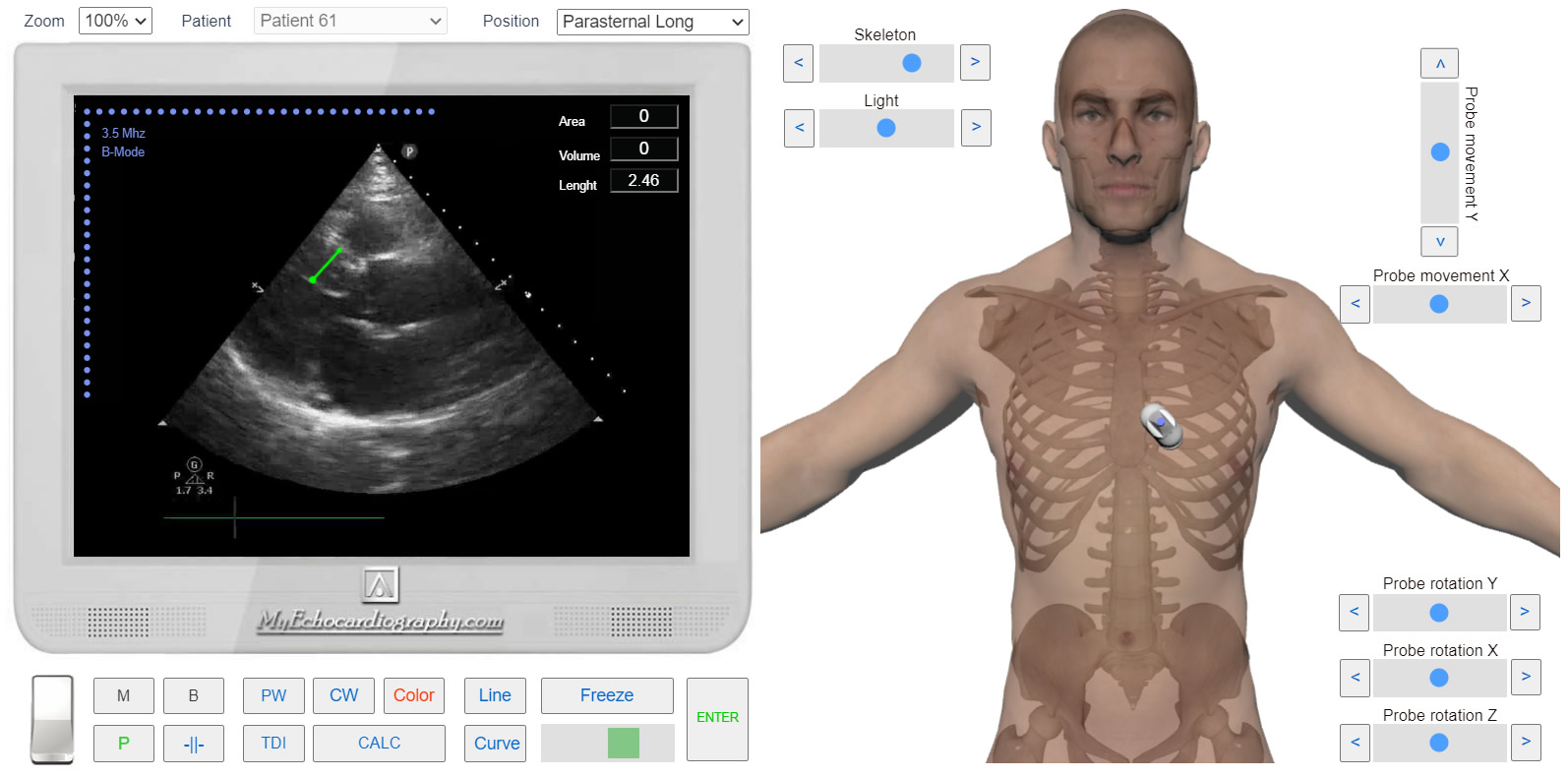
Left parasternal View, long axis. Hypertrophic Cardiomyopathy. Simulation By Echocardiography Online Simulator MyEchocardiography.com
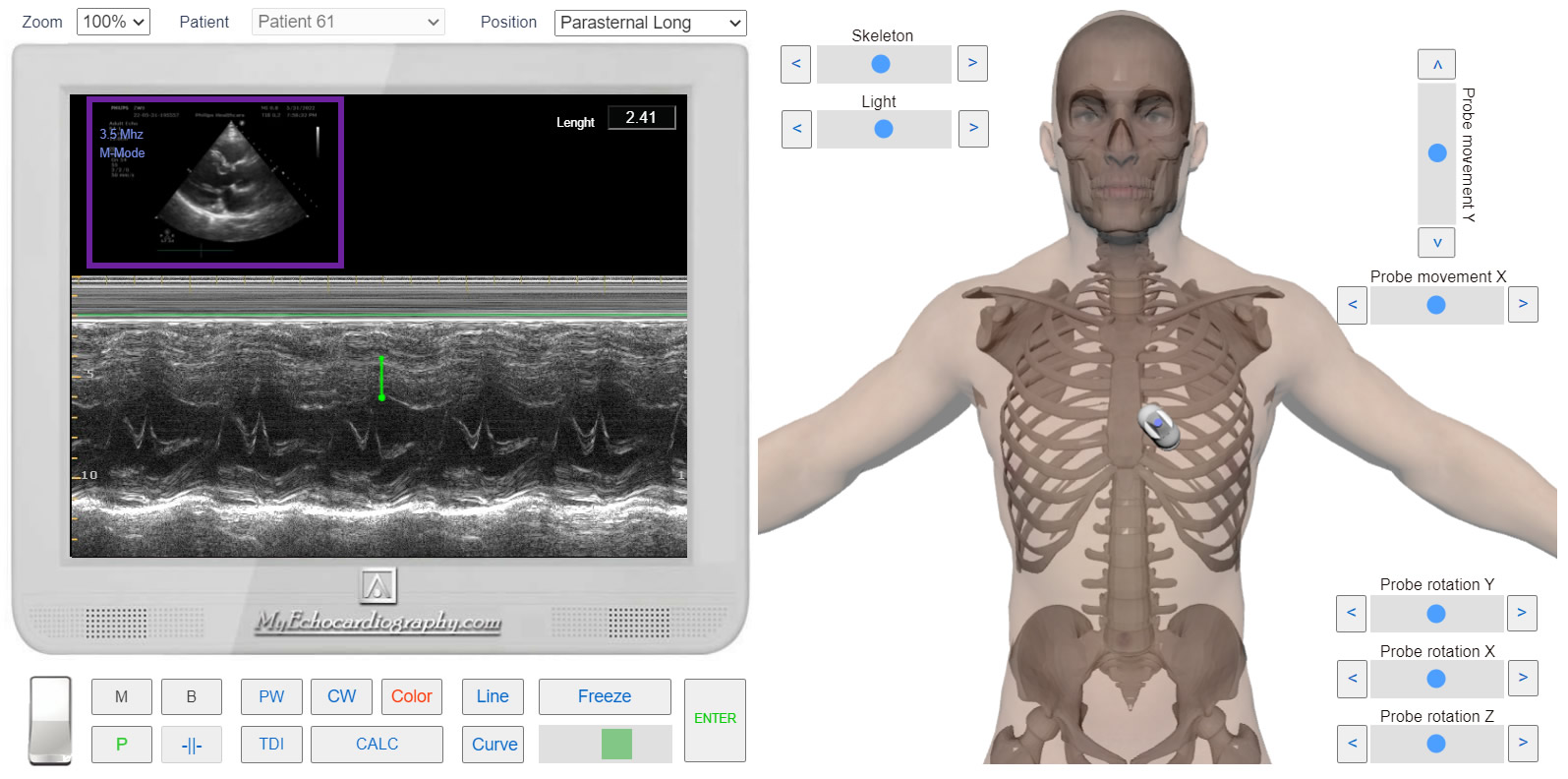
Left parasternal View, long axis. M-mode. Hypertrophic Cardiomyopathy. Simulation By Echocardiography Online Simulator MyEchocardiography.com
Simulate Hypertrophic Cardiomyopathy >>>